Understanding and Creating Comprehensive Soap Notes in Healthcare
Creating effective soap notes is crucial for clear and efficient communication within healthcare teams. Soap notes (Subjective, Objective, Assessment, Plan) provide a structured format for documenting patient encounters, ensuring all relevant information is captured and communicated clearly among providers. This guide aims to provide you with detailed, actionable advice to master soap note writing, along with real-world examples and practical solutions to common issues. Let’s dive into the essential elements of creating comprehensive soap notes that will help you meet your users’ needs efficiently.
Soap notes are often used in various healthcare settings including primary care, nursing, mental health, and more. The structure aids in organizing information systematically, making it easier for healthcare professionals to follow and for patients to understand their treatment plans. This guide will focus on guiding you through the entire soap note process, from basic to advanced levels, ensuring that you can implement these skills in your daily practice.
Quick Reference Guide
Quick Reference
- Immediate action item with clear benefit: Start by documenting the patient’s chief complaint in the subjective section to ensure you’re addressing their main concern. This will guide the rest of the note and focus the care plan.
- Essential tip with step-by-step guidance: Break down your observations into clear, concise, and objective data for the objective section. For example, when recording vital signs, make sure to include temperature, blood pressure, heart rate, and respiratory rate, noting any abnormalities clearly.
- Common mistake to avoid with solution: Avoid including too much subjective data in the objective section. Stick to factual observations and leave detailed patient narratives for the subjective section to avoid confusion.
Step-by-Step Guidance to Create a Soap Note
Let’s break down each section of a soap note and provide you with detailed instructions to master this essential documentation tool:
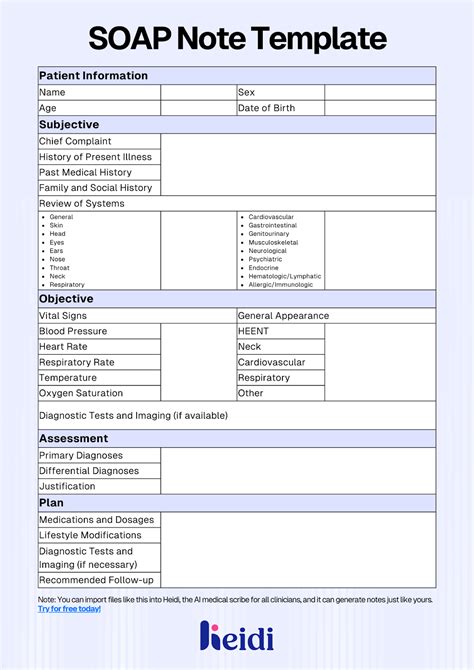
Subjective Section
The subjective section is where you document the patient’s personal account of their health concerns. It’s all about what the patient says and feels. Here’s how to write it effectively:
- Chief Complaint: Start with a concise statement of the reason for the patient's visit. For example, “Patient reports a 3-day history of a sore throat and difficulty swallowing.”
- History of Present Illness (HPI): Provide a detailed narrative describing the symptom’s onset, duration, intensity, and any factors that alleviate or exacerbate it. For example, “The sore throat began three days ago and has progressively worsened, causing discomfort especially when swallowing. The patient rates the pain as 7/10. No relief with over-the-counter medications.
- Past Medical History (PMH): Include any relevant medical history, such as previous diagnoses or chronic conditions that might influence the current issue. For example, “Patient has a history of strep throat diagnosed two years ago.”
- Medications: List all medications the patient is currently taking, including dosages and frequencies. For example, “The patient is currently on ibuprofen 200 mg every 6 hours for pain relief.”
- Allergies: Document any known drug, food, or environmental allergies, and their reactions. For example, “Allergic to penicillin; reaction includes rash and swelling.”
Objective Section
The objective section includes factual, observable data and is purely objective. Here’s how to document effectively:
- Vital Signs: Record essential measurements such as blood pressure, heart rate, respiratory rate, temperature, and oxygen saturation. For example, “BP: 120/80 mmHg, HR: 90 bpm, RR: 18 breaths per minute, Temp: 37.5°C, O2 sat: 98% on room air.”
- Physical Examination: Provide a detailed description of the physical exam findings. For example, “Throat exam reveals erythema of the tonsils with exudate and mild swelling of the cervical lymph nodes.”
- Diagnostic Tests: Include results from any diagnostic tests performed, such as lab results or imaging studies. For example, “Rapid strep test positive.”
- Assessment: Summarize the clinical impression based on subjective and objective data. For example, “Patient presents with signs and symptoms consistent with acute streptococcal pharyngitis.”
Practical FAQ
How do I ensure my soap note is comprehensive yet concise?
To balance thoroughness and brevity, focus on:
- Relevance: Include only pertinent information that directly relates to the patient’s current issue.
- Clarity: Use clear, concise language without jargon to make it easily understandable for all healthcare providers.
- Consistency: Follow a standard format to ensure all necessary information is included without unnecessary details.
What should I include in the assessment section?
The assessment section should include:
- Diagnosis: Your clinical impression based on subjective and objective data.
- Differential Diagnosis: Consider other possible conditions and why they were ruled out.
- Plan: The next steps in the care plan should directly follow the diagnosis.
How can I avoid common errors in soap note writing?
Common errors include:
- Incomplete Data: Always complete the subjective and objective sections fully before moving to assessment and plan.
- Lack of Clarity: Avoid ambiguous terms. Use specific terms to describe symptoms and findings.
- Confusing Subjective and Objective Sections: Keep subjective information patient narratives and objective information as factual observations.
By following these steps and tips, you can create soap notes that are not only thorough and professional but also beneficial for patient care and communication across the healthcare team. Start mastering these skills today to enhance your practice and patient outcomes.
Remember, a well-structured soap note is a valuable tool in the healthcare arsenal, ensuring that all healthcare providers have a clear, shared understanding of the patient’s condition and treatment plan. Practice these steps regularly to build competence and confidence in your documentation abilities.


